
Apr 15 2016
Neural Bypass Helps Quadriplegic Man Use His Arm
 I have been following and writing about the development of neural prosthetics and brain-machine interfaces as the technology has been advancing over the last decade. These are techniques that read electrical signals from the brain, process those signals through a computer algorithm, and use them to control some external device.
I have been following and writing about the development of neural prosthetics and brain-machine interfaces as the technology has been advancing over the last decade. These are techniques that read electrical signals from the brain, process those signals through a computer algorithm, and use them to control some external device.
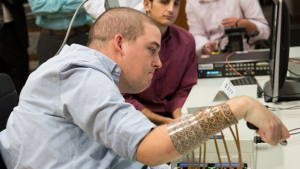
Another milestone has been reached in this technology. Researchers at Ohio State University implanted electrodes on the motor cortex of a man with a mid cervical quadriplegia. He cannot use his hands or legs. The output from these electrodes was then connected to a sleeve over his right forearm that could electrically stimulate his muscles in specific patterns to produce useful movements, like grasping and releasing.
After several hours of practice:
The system provided isolated finger movements and the participant achieved continuous cortical control of six different wrist and hand motions. Furthermore, he was able to use the system to complete functional tasks relevant to daily living.
While control was pretty basic, what is important is the specific functions that the subject could perform. Even the ability to do a simple grasp has enormous consequences for daily activities – such as feeding oneself, brushing your teeth, other grooming activity, and opening doors.
Researchers have already been able to implant electrodes in non-human primates and teach them to operate a robotic arm. Surface electrodes have also been used in humans allowing for a basic level of computer control.
This new demonstration is a baby step forward, but it does show the clinical potential of this technology in paralyzed people.
Here are some limitations, however. The electrodes are implanted on the brain. It remains to be seen how long these electrodes will function, if they will move, if scar tissue will form, or they will stop working for some other reason.
The electrodes need to connect to a computer and then to a rather bulky sleeve on the forearm. This is a minor hindrance, especially for someone in a wheelchair, and is probably the easiest aspect of this technology to improve over time.
The muscles are stimulated from the outside through the skin. This works just fine. Muscles are electrical organs and will respond to external stimulation. The resolution of the stimulation is limited by this technique, but the study shows it is adequate to give a functional level of control.
However, external stimulation will not replace the effects of normal nerve supply. What this means is that, for a lower motor neuron lesion (the motor neuron that connects to the muscle) atrophy will still occur. Nerve supply keeps muscle fibers healthy, and external stimulation does not replace nerve supply. For upper motor neuron lesions (the neuron from the brain down to the spinal cord) the big problem is spasticity, the muscle contracts involuntarily because it is missing the inhibitory tone from the upper motor neuron. External stimulation also does not solve this problem.
Spasticity can be so severe that the hand becomes frozen in a clenched position, unable to open. Regular movement of the hand, however, is helpful in preventing these contractions. This is accomplished with occupational therapy and splints, but a neural prosthetic that allows for voluntary movement might help also. This remains to be seen.
In other words, this system is a meaningful advance, and will likely find applications in some patients. But this is not a perfect solution and will not work for everyone. We now also need to see what the lifespan of this technology is.
This is not a radical new approach but a baby step, an application of technology that has been developing for years. It is exciting to watch as this technology unfolds, however, and we are now seeing the beginning of its clinical potential.




