
May 29 2020
The Learning Styles Myth
I have written previously about the fact that the scientific evidence does not support the notion that different people have different inherent learning styles. Despite this fact, the concept remains popular, not only in popular culture but among educators. For fun a took the learning style self test at educationplanner.org. It was complete nonsense. I felt my answer to all the forced-choice questions was “it depends.” In the end I scored 35% visual, 35% auditory, and 30% kinesthetic, from which the site concluded I was a visual-auditory learner.
about the fact that the scientific evidence does not support the notion that different people have different inherent learning styles. Despite this fact, the concept remains popular, not only in popular culture but among educators. For fun a took the learning style self test at educationplanner.org. It was complete nonsense. I felt my answer to all the forced-choice questions was “it depends.” In the end I scored 35% visual, 35% auditory, and 30% kinesthetic, from which the site concluded I was a visual-auditory learner.
Clearly we need to do a better job of getting the word out there – forget learning styles, it’s a dead end. The Yale Poorvu Center for Teaching and Learning has done a nice job of summarizing why learning styles is a myth, and makes a strong case for why the concept is counterproductive.
The idea is that individual people learn better if the material is presented in a style, format, or context that fits best with their preferences. The idea is appealing because, first, everyone likes to think about themselves and have something to identify with. But also it gives educators the feeling that they can get an edge by applying a simple scheme to their teaching. I also frequently find it is a convenient excuse for lack of engagement with material.
There are countless schemes for separating the world into a limited number of learning styles. Perhaps the most popular is visual, auditory, vs kinesthetic. But there are many, and the Yale site lists the most popular. They include things such as globalists vs. analysts, assimilators vs. accommodators, imaginative vs. analytic learners, non-committers vs. plungers. If you think this is all sounding like an exercise in false dichotomies, I agree.
Regardless of why people find the notion appealing, or which system you prefer, the bottom line is that the basic concept of learning styles is simply not supported by scientific evidence.
 Human thought processes are powerful but flawed, like a GPS system that uses broken algorithms to lead you to the wrong destination. Psychologists study these cognitive biases and heuristic patterns of thought to better understand these flaws and propose possible fixes to mitigate them. To a large degree, scientific skepticism is about exactly that – identifying and compensating for the flaws in human cognition.
Human thought processes are powerful but flawed, like a GPS system that uses broken algorithms to lead you to the wrong destination. Psychologists study these cognitive biases and heuristic patterns of thought to better understand these flaws and propose possible fixes to mitigate them. To a large degree, scientific skepticism is about exactly that – identifying and compensating for the flaws in human cognition. Is someone’s basic personality type written on their face? This is an interesting question, that research has not definitively answered.
Is someone’s basic personality type written on their face? This is an interesting question, that research has not definitively answered. 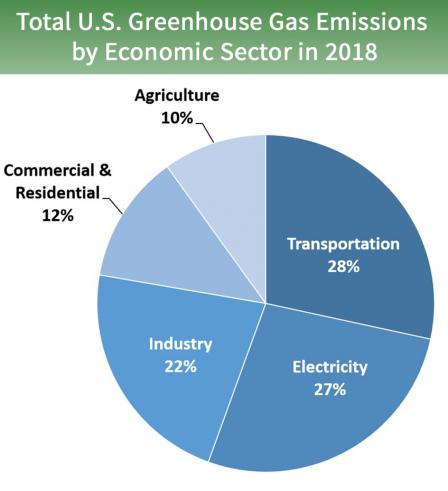 Here is a tiny bit of good news on the climate change front:
Here is a tiny bit of good news on the climate change front: 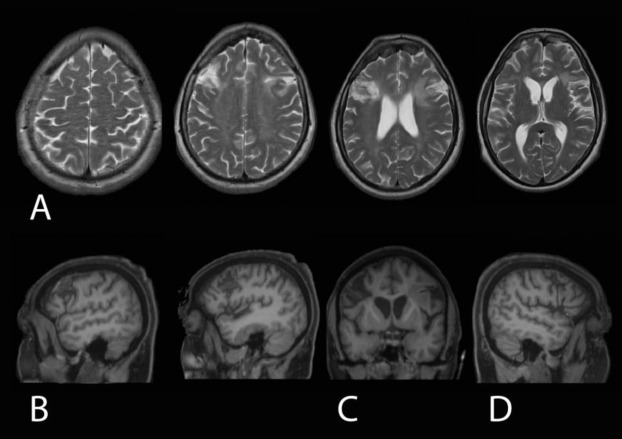 Where in the brain is a specific ability located? This is a more complex question than it may at first seem, mainly because we first have to define each specific ability. Some are obvious, like the ability to voluntarily move your right hand. The motor strip in the cortex physically maps to the body, and it is relatively easy to correlate a specific part of the brain to weakness of any specific body part. But even something as simple as motor control has many layers – other parts of the brain that modify control, allowing for smooth coordinated movement, for example.
Where in the brain is a specific ability located? This is a more complex question than it may at first seem, mainly because we first have to define each specific ability. Some are obvious, like the ability to voluntarily move your right hand. The motor strip in the cortex physically maps to the body, and it is relatively easy to correlate a specific part of the brain to weakness of any specific body part. But even something as simple as motor control has many layers – other parts of the brain that modify control, allowing for smooth coordinated movement, for example. A new study
A new study 
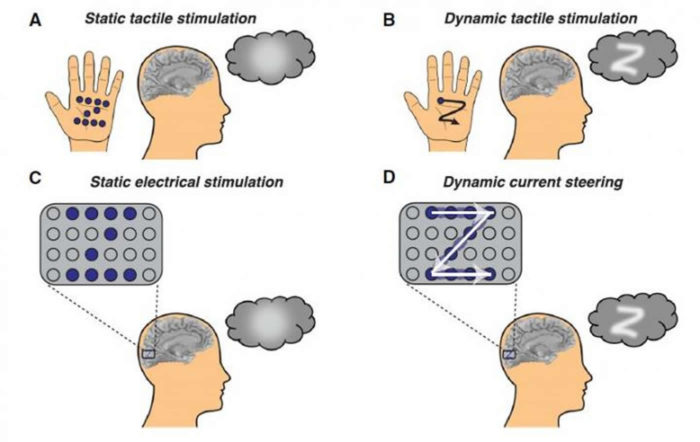 For adults who had vision but then lose it due to eye disease or damage to the optic nerve, their visual cortex is still intact. It is deprived if input, but is theoretically capable of functioning normally to create images. The ultimate technological expression of this potential would be something like the visor of Geordi La Forge – a device that can see (even in frequencies and particles humans cannot normally see) and transfer that information to the visual cortex. Obviously we are a long way away from any such technology, but we have taken the first baby steps in that direction, including a recent study which makes one tiny advance (but more on that shortly).
For adults who had vision but then lose it due to eye disease or damage to the optic nerve, their visual cortex is still intact. It is deprived if input, but is theoretically capable of functioning normally to create images. The ultimate technological expression of this potential would be something like the visor of Geordi La Forge – a device that can see (even in frequencies and particles humans cannot normally see) and transfer that information to the visual cortex. Obviously we are a long way away from any such technology, but we have taken the first baby steps in that direction, including a recent study which makes one tiny advance (but more on that shortly). Perhaps one of the positive outcomes of the pandemic is an acceleration of acceptance of telehealth and telementalhealth – treating patients online instead of in person. For example, we have been trying to institute telehealth where I work for years, but have met with roadblocks. Then, all of a sudden, we were able to do it. Our clinic manager estimates that we accomplished in three weeks what would have otherwise taken three years. I have been doing mostly telehealth visits for the last two months now. It’s not perfect, but for many patients it is an ideal option.
Perhaps one of the positive outcomes of the pandemic is an acceleration of acceptance of telehealth and telementalhealth – treating patients online instead of in person. For example, we have been trying to institute telehealth where I work for years, but have met with roadblocks. Then, all of a sudden, we were able to do it. Our clinic manager estimates that we accomplished in three weeks what would have otherwise taken three years. I have been doing mostly telehealth visits for the last two months now. It’s not perfect, but for many patients it is an ideal option.




