Feb
26
2026
 The news is abuzz with talk of a potential universal respiratory vaccine. It’s definitely interesting research, but may not be what you think. In this case, the reporting has been quite good on the whole, but the headlines can be misleading if you are not deeply steeped in the complexities of mammalian immunity. Let me start with the biggest caveat – this is a mouse study. This is therefore encouraging pre-clinical research, but we are still years away from translating this into an actual vaccine. Also, most interventions that are encouraging at the animal stage don’t make it through human testing. So don’t expect any revolution based on this treatment anytime soon. Having said that – there is great potential here.
The news is abuzz with talk of a potential universal respiratory vaccine. It’s definitely interesting research, but may not be what you think. In this case, the reporting has been quite good on the whole, but the headlines can be misleading if you are not deeply steeped in the complexities of mammalian immunity. Let me start with the biggest caveat – this is a mouse study. This is therefore encouraging pre-clinical research, but we are still years away from translating this into an actual vaccine. Also, most interventions that are encouraging at the animal stage don’t make it through human testing. So don’t expect any revolution based on this treatment anytime soon. Having said that – there is great potential here.
To understand how this new approach works, let’s review some basics of immunity. (Note – the immune system is incredibly complex, and I can only give a very superficial summary here, but enough to understand what’s going on.) Mammalian immune systems have two basic components, innate immunity and adaptive immunity. The adaptive immune system is probably what most people think about when they think about the immune system and vaccines. Adaptive immunity targets and recognizes specific antigens (such as proteins) on pathogens like viruses, bacteria, or fungi. Antibodies attach to these antigens, flagging them to be targeted by immune cells like macrophages which then eat them. The macrophages in turn display the antibody-flagged antigens on their surface, triggering a greater and more specific reaction to those specific antigens. Adaptive immunity is considered slow (it takes days to ramp up), specific (it targets specific antigens on specific pathogens) and durable (it has memory, and will react more quickly and robustly to the same pathogen in the future).
By contrast, the innate immune system is fast, non-specific, and short-lived with no memory. The innate immune system consists of physical barriers, like skin and mucosa, and immune cells that target pathogens based on broad patterns that are not learned but are innate (hence the name). There are Toll-like receptors (TLRs – the name Toll comes from the German for “fantastic”, allegedly said by a researcher upon discovery). The Toll gene was first discovered in fruit flies and then similar genes were later discovered in mammals, hence “Toll-like”. TLRs detect pathogen-associated molecular patterns (PAMPs), which are highly conserved features of types of pathogens. In other words – a TLR might recognize a snippet of RNA as a pattern typical of RNA viruses, or proteins that tend to occur on pathogenic bacteria. “That looks like an RNA virus, so let’s attack it.”
Continue Reading »
Dec
08
2025
A new study reinforces the evidence for the safety and efficacy of the mRNA COVID-19 vaccines. That’s the TLDR, but let’s dive into the details.
reinforces the evidence for the safety and efficacy of the mRNA COVID-19 vaccines. That’s the TLDR, but let’s dive into the details.
Medical evidence is always rolled out in stages. First there is what we would consider preclinical evidence, or basic science. This could be initial uncontrolled clinical observations, or mechanistic animal or in vitro research. At some point we have sufficient evidence to generate a hypothesis that a specific treatment could be effective in treating a specific disease, enough to progress to human research. For FDA qualifying research, there are four specific phases. Phase I trials look at the safety of the intervention in usually healthy controls, while also answering basic questions and mechanism and effects. If there are no safety red-flags then the research progressed to a phase II trial, which look for preliminary evidence of efficacy, and further safety data. Again, if that data continues to look encouraging we can progress to a phase III trial, which is a larger and more rigorous trial designed to be definitive. Usually the FDA requires several phase III trials to grant approval of a drug for a specific indication. Then, once on the market there is phase IV trials, which look at data from more widespread use to confirm safety and effectiveness in the real world.
Looked at another way, we do research in the lab, then on dozens of people, then score to hundreds of people, then hundreds to thousands of people, and then finally on thousands to millions of people. Each step of the way we gain the ability to detect less and less common side effects in a broader set of people. Further, the types of evidence are designed to be complementary. Phase III trials, for example, are rigorously experimental, with highly defined populations with randomization to control as many variables as possible. Phase IV trials, on the other hand, are generally observational, designed to look at very large numbers of people in an uncontrolled setting – to determine how safe and effective the treatment is in real-world conditions.
Continue Reading »
Sep
23
2025
 Yesterday, Trump and RFK Jr had a press conference which some are characterizing as the absolutely worst firehose of medical misinformation coming from the White House in American history. I think that is fair. This was the presser we knew was coming, and many of us were dreading. It was worse than I anticipated.
Yesterday, Trump and RFK Jr had a press conference which some are characterizing as the absolutely worst firehose of medical misinformation coming from the White House in American history. I think that is fair. This was the presser we knew was coming, and many of us were dreading. It was worse than I anticipated.
I suspect much of this stems from RFKs previous promise that in six months he would find the cause of autism so that we can start eliminating these exposures – six months is September. This was an absurd claim given that there has been and continues to be extensive international research into autism for decades, and absolutely no reason to suspect any major breakthrough in those six months. Those of us following RFK’s career knew what he meant – he believes he already knows the causes, that they are environmental (hence “exposures”) and include vaccines.
So Kennedy had to gin up some big autism announcement this month, and there is always plenty of preliminary or inconclusive research going on that you can cherry pick to support some preexisting narrative. It was basically leaked that his target was going to be an alleged link between Tylenol (acetaminophen) use in pregnancy and autism. This gave us an opportunity to pre-debunk this claim, which many did. Just read my linked article in SBM to review the evidence – bottom line, there is no established cause and effect and two really good reasons to doubt one exists: lack of a dose response curve, and when you control for genetics, any association vanishes.
Continue Reading »
Jun
26
2025

RFK Jr. is an anti-vaxxer. He will protest that, but it’s a dodge. He basically lied (and it was quite transparent) to the senate confirmation committee, and I think Cassidy and others knew full well what they were getting when they approved him as HHS secretary. Those of us who have been following RFK’s career as an anti-vaxxer have not been surprised (although we are certainly horrified) as he got to work systematically undermining vaccines in every way within his reach. You can read the saga in great detail at SBM, where we anticipated his moves. Let’s quickly review.
Of course, RFK is not going to say, “I will destroy America’s vaccine infrastructure because I hate all vaccines.” He is doing what he always does, using a pretext. Now he is claiming that he is just supporting “gold standard science”. But this is exactly like science deniers saying that they are just applying healthy skepticism. When it comes to safety data, for example, you can set the bar as arbitrarily high as you want. There is no such thing as 100% certitude in science or medicine, and so you can nit pick the evidence-base and declare that any medical intervention you don’t like needs more safety data. You can claim that any connection to industry is a fatal conflict of interest, even if it isn’t. You can claim data is too old and needs review, or that public funds are better spent elsewhere. Finding a pretext to undermine vaccines is easy. The pattern, however, is undeniable and was predicted – in every case, RFK’s judgement will come down against vaccines.
He has pulled funding for mRNA research into viruses with pandemic potential, including the bird flu. He clawed back funding that was already given to fund testing, claiming the vaccine needs more testing. he also claimed that other interventions are more promising. This, of course, is also the guy who thinks that vitamin A is more effective than vaccines at preventing measles, something which is patently not true. It’s hard to imagine a better health investment than developing a vaccine to prevent the next pandemic, but here we are.
Continue Reading »
Jun
06
2025
 First, don’t get too excited, this is a laboratory study, which means if all goes well we are about a decade or more from an actual treatment. The study, however, is a nice demonstration of the potential of recent biotechnology, specifically mRNA technology and lipid nanoparticles. We are seeing some real benefits building on decades of basic science research. It is a hopeful sign of the potential of biotechnology to improve our lives. It is also a painful reminder of how much damage is being done by the current administration’s defunding of that very science and the institutions that make it happen.
First, don’t get too excited, this is a laboratory study, which means if all goes well we are about a decade or more from an actual treatment. The study, however, is a nice demonstration of the potential of recent biotechnology, specifically mRNA technology and lipid nanoparticles. We are seeing some real benefits building on decades of basic science research. It is a hopeful sign of the potential of biotechnology to improve our lives. It is also a painful reminder of how much damage is being done by the current administration’s defunding of that very science and the institutions that make it happen.
The study –Efficient mRNA delivery to resting T cells to reverse HIV latency – is looking for a solution to a particular problem in the treatment of HIV. The virus likes to hide inside white blood cells (CD4+ T cells). There the virus will wait in a latent stage and can activate later. It acts as a reservoir of virus that can keep the infection going, even in the face of effective anti-HIV drugs and immune attack. It is part of what makes HIV so difficult to fully eliminate from the body.
We already have drugs that address this issue. They are called, appropriately, latency-reversing agents (LRAs), and include Romidepsin, Panobinostat, and Vorinostat. These drugs inhibit an enzyme which allows the virus to hide inside white blood cells. So this isn’t a new idea, and there are already effective treatments, which do make other anti-HIV drugs more effective and keep viral counts very low. But they are not quite effective enough to allow for total virus elimination. More and more effective LRAs, therefore, could be highly beneficial to HIV treatment.
Continue Reading »
May
06
2025
The recent discussions about autism have been fascinating, partly because there is a robust neurodiversity community who have very deep, personal, and thoughtful opinions about the whole thing. One of the issues that has come up after we discussed this on the SGU was that of self-diagnosis. Some people in the community are essentially self-diagnosed as being on the autism spectrum. Cara and I both reflexively said this was not a good thing, and then moved on. But some in the community who are self-diagnosed took exception to our dismissiveness. I didn’t even realize this was a point of contention.
Two issues came up, the reasons they feel they need self-diagnosis, and the accuracy of self diagnosis. The main reason given to support self-diagnoses was the lack of adequate professional services available. It can be difficult to find a qualified practitioner. It can take a long time to get an appointment. Insurance does not cover “mental health” services very well, and so often getting a professional diagnosis would simply be too expensive for many to afford. So self-diagnosis is their only practical option.
I get this, and I have been complaining about the lack of mental health services for a long time. The solution here is to increase the services available and insurance coverage, not to rely on self-diagnosis. But this will not happen overnight, and may not happen anytime soon, so they have a point. But this doesn’t change the unavoidable reality that diagnoses based upon neurological and psychological signs and symptoms are extremely difficult, and self-diagnosis in any medical area is also fraught with challenges. Let me start by discussing the issues with self-diagnosis generally (not specifically with autism).
I wrote recently about the phenomenon of diagnosis itself. (I do recommend you read that article first, if you haven’t already.) A medical/psychological diagnosis is a complex multifaceted phenomenon. It exists in a specific context and for a specific purpose. Diagnoses can be purely descriptive, based on clinical signs and symptoms, or based on various kinds of biological markers – blood tests, anatomical scans, biopsy findings, functional tests, or genetics. Also, clinical entities are often not discrete, but are fuzzy around the edges, manifest differently in different populations and individuals, and overlap with other diagnoses. Some diagnoses are just placeholders for things we don’t understand. There are also generic categorization issues, like lumping vs splitting (do we use big umbrella diagnoses or split every small difference up into its own diagnosis?).
Continue Reading »
Apr
29
2025
In my previous post I wrote about how we think about and talk about autism spectrum disorder (ASD), and how RFK Jr misunderstands and exploits this complexity to weave his anti-vaccine crank narrative. There is also another challenge in the conversation about autism, which exists for many diagnoses – how do we talk about it in a way that is scientifically accurate, useful, and yet not needlessly stigmatizing or negative? A recent NYT op-ed by a parent of a child with profound autism had this to say:
“Many advocacy groups focus so much on acceptance, inclusion and celebrating neurodiversity that it can feel as if they are avoiding uncomfortable truths about children like mine. Parents are encouraged not to use words like “severe,” “profound” or even “Level 3” to describe our child’s autism; we’re told those terms are stigmatizing and we should instead speak of “high support needs.” A Harvard-affiliated research center halted a panel on autism awareness in 2022 after students claimed that the panel’s language about treating autism was “toxic.” A student petition circulated on Change.org said that autism ‘is not an illness or disease and, most importantly, it is not inherently negative.'”
I’m afraid there is no clean answer here, there are just tradeoffs. Let’s look at this question (essentially, how do we label ASD) from two basic perspectives – scientific and cultural. You may think that a purely scientific approach would be easier and result in a clear answer, but that is not the case. While science strives to be objective, the universe is really complex, and our attempts at making it understandable and manageable through categorization involve subjective choices and tradeoffs. As a physician I have had to become comfortable with this reality. Diagnoses are often squirrelly things.
When the profession creates or modifies a diagnosis, this is really a type of categorization. There are different criteria that we could potentially use to define a diagnostic label or category. We could use clinical criteria – what are the signs, symptoms, demographics, and natural history of the diagnosis in question? This is often where diagnoses begin their lives, as a pure description of what is being seen in the clinic. Clinical entities almost always present as a range of characteristics, because people are different and even specific diseases will manifest differently. The question then becomes – are we looking at one disease, multiple diseases, variations on a theme, or completely different processes that just overlap in the signs and symptoms they cause. This leads to the infamous “lumper vs splitter” debate – do we tend to lump similar entities together in big categories or split everything up into very specific entities, based on even tiny differences?
Continue Reading »
Jul
02
2024
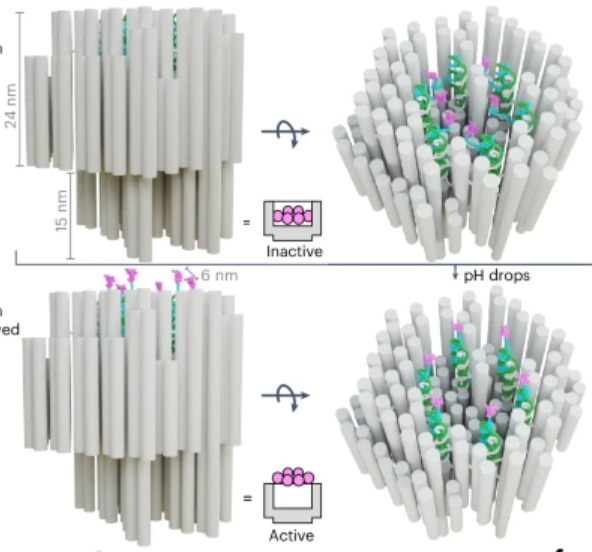 How’s that for a provocative title? But it is technically accurate. The title of the paper in question is: “A DNA robotic switch with regulated autonomous display of cytotoxic ligand nanopatterns.” The study is a proof of concept in an animal model, so we are still years away from a human treatment (if all goes well), but the tech is cool.
How’s that for a provocative title? But it is technically accurate. The title of the paper in question is: “A DNA robotic switch with regulated autonomous display of cytotoxic ligand nanopatterns.” The study is a proof of concept in an animal model, so we are still years away from a human treatment (if all goes well), but the tech is cool.
First we start with what is called “DNA origami”. These are sequences of DNA that fold up into specific shapes. In this case the DNA origami is used to create a nanoscale “robot” which is used as a delivery mechanism for the kill switch. The skill switch is quite literal – a “death receptor” (DR) which is a ligand of 6 amino acids. These exist on all healthy cells, but when sufficiently clustered on the surface of a cell, DRs trigger apoptosis, which is programmed cell death – a death switch.
The DNA origami robot has six such ligands arranged in a hexagonal pattern on the interior of its structure. The DNA, in fact, creates this structure with precise distance and arrangement to effectively trigger apoptosis. When it opens up it reveals these ligands and can attach them to a cell surface, triggering apoptosis. The researchers have managed to create a DNA robot that remains closed in normal body pH, but also will open up in an acidic environment.
Continue Reading »
Mar
25
2024
 On March 16 surgeons transplanted a kidney taken from a pig into a human recipient, Rick Slayman. So far the transplant is a success, but of course the real test will be how well the kidney functions and for how long. This is the first time such a transplant has been done into a living donor – previous experimental pig transplants were done on brain dead patients.
On March 16 surgeons transplanted a kidney taken from a pig into a human recipient, Rick Slayman. So far the transplant is a success, but of course the real test will be how well the kidney functions and for how long. This is the first time such a transplant has been done into a living donor – previous experimental pig transplants were done on brain dead patients.
This approach to essentially “growing organs” for transplant into humans, in my opinion, has the most potential. There are currently over 100 thousand people on the US transplant waiting list, and many of them will die while waiting. There are not enough organs to go around. If we could somehow manufacture organs, especially ones that have a low risk of immune rejection, that would be a huge medical breakthrough. Currently there are several options.
One is to essentially construct a new organ. Attempts are already underway to 3D print organs from stem cells, which can be taken from the intended recipient. This requires a “scaffold” which is connective tissue taken from an organ where the cells have been stripped off. So you still need, for example, a donor heart. You then strip that heart of cells, 3D print new heart cells onto what’s left to create a new heart. This is tricky technology, and I am not confident it will even work.
Another option is to grow the organs ex-vivo – grow them in a tank of some kind from stem cells taken from the intended recipient. The advantage here is that the organ can potentially be a perfect new organ, entirely human, and with the genetics of the recipient, so no issues with rejection. The main limitation is that it takes time. Considering, however, that people often spend years on the transplant wait list, this could still be an option for some. The problem here is that we don’t currently have the technology to do this.
Continue Reading »
Feb
16
2024
 I was recently asked what I thought about the Solex AO Scan. The website for the product includes this claim:
I was recently asked what I thought about the Solex AO Scan. The website for the product includes this claim:
AO Scan Technology by Solex is an elegant, yet simple-to-use frequency technology based on Tesla, Einstein, and other prominent scientists’ discoveries. It uses delicate bio-frequencies and electromagnetic signals to communicate with the body.
The AO Scan Technology contains a library of over 170,000 unique Blueprint Frequencies and created a hand-held technology that allows you to compare your personal frequencies to these Blueprints in order to help you achieve homeostasis, the body’s natural state of balance.
This is all hogwash (to use the technical term). Throwing out the names Tesla and Einstein, right off, is a huge red flag. This is a good rule of thumb – whenever these names (or Galileo) are invoked to hawk a product, it is most likely a scam. I guess you can say that any electrical device is based on the work of any scientist who had anything to do with electromagnetism.
Continue Reading »





